What are lacerations and episiotomies: everything you need to know

Pregnancy is a period that involves many expectations, achievements, and also some fears. Among the main fears, the occurrence of lacerations during vaginal delivery has been keeping women awake at night, as well as the need or not to perform an episiotomy.
It is very common during normal delivery for some type of tear in the skin or even muscles to occur in order for the baby to come out. On average, 53% to 79% of women report having suffered this tear, even if it is minor.
The main problem with tearing is when it also ruptures the anus. To “facilitate” delivery and avoid this tearing, there is the episiotomy, which is a cut made in the opening of the vaginal canal to increase the space available for the baby to pass through. It has become a common practice and, at the same time, somewhat controversial.
What is the difference between a laceration and an episiotomy?
The difference between a laceration and an episiotomy is a frequent question throughout pregnancy.
- A perineal laceration (or tearing) is nothing more than a natural tear in the tissue of the birth canal, more specifically in the perineal area, during the delivery of the baby. It can occur for several reasons, but the main one is due to the size of the baby’s head. In this case, it is usually larger than the birth canal, and as it passes through the pelvis and the tissues are stretched, it can cause injury.
- An episiotomy is precisely the cut that doctors usually make to prevent a serious laceration from occurring. Its main indication is to prevent laceration of the anus. It is performed with a scalpel, cutting the skin and muscles of the vulva, preferably on the side, to prevent laceration of the anus during the baby’s delivery. Afterwards, everything is properly sutured.
The great controversy surrounding episiotomy is that it is not necessary in all situations because severe laceration does not always occur. However, some professionals end up suggesting the procedure even to speed up delivery, unnecessarily imposing on women the consequences that this cut offers later.
Categories of laceration
Lacerations can be classified into degrees, depending on the area affected by the cut and its severity:
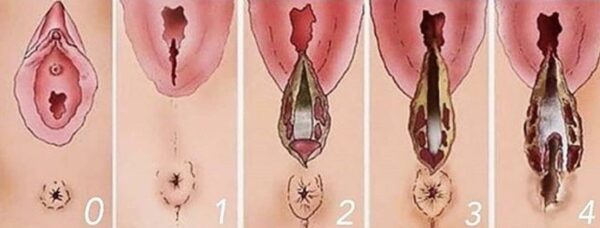
- 1st degree: In the mildest lacerations, only the labia minora, vaginal mucosa, or superficial skin of the perineum are usually affected. The cut usually heals naturally, sometimes without the need for stitches;
- 2nd degree: In addition to affecting the areas mentioned in 1st degree lacerations, it affects the perineal muscles and fascia, which is the fibrous tissue that attaches some muscles. In this type of injury, stitches are usually recommended to aid healing.
- 3rd degree: In addition to the areas already mentioned, there is also laceration of the anal sphincter, regardless of whether the cut is superficial or tears it internally. In this case, it is important to take some precautions and reconstruct the sphincter with stitches during delivery so that its restructuring occurs quickly. In some cases, rehabilitation with pelvic floor physical therapy is also necessary.
- 4th degree: This most severe level of laceration occurs when, in addition to all the areas affected in the other degrees, it affects the anal mucosa. This is the most critical degree and, therefore, it is essential to take all necessary precautions.
Although perineal lacerations toward the anus are the most common, cuts can occur in other places, such as near the urethra, at the top of the vagina. Called a periurethral laceration, it is usually small and does not reach the muscle, making it less painful and healing faster, requiring only a few stitches.
There are cases of cervical rupture that must also be reconstructed immediately after delivery.
What are the causes and consequences of laceration?
There are several reasons that can lead to laceration, since it is a sensitive area that requires enlargement for delivery to occur.
In general, the main risk factors are:
- First vaginal delivery;
- Second vaginal delivery in which the previous delivery already caused injury;
- Very large baby;
- Very small distance between the anus and the vaginal opening;
- When delivery occurs very quickly;
- When there is no preparation of the perineum during pregnancy.
Laceration can also occur even with an episiotomy, as if the cut were to widen due to the effort or size of the baby, or even in other places.
This rupture does not usually cause very serious long-term problems, especially when it occurs at milder levels. However, those who have had a grade three or four problem may have more serious sequelae.
Although rare, the main complaints reported by women after laceration are:
- Urinary and fecal incontinence;
- Urgency to go to the bathroom;
- Chronic perineal pain;
- Pain during sexual intercourse.
In what cases is an episiotomy indicated?
As it is a surgical procedure, an episiotomy should be performed with caution and only when truly necessary.
Many doctors find it difficult to know when the perineum is actually at risk of tearing, and to avoid laceration, they end up performing an episiotomy. However, the World Health Organization states that the technique should only be used in specific cases, especially when there is a risk to the mother.
Thus, a scalpel incision is recommended when:
- There is a chance of severe laceration (grade 3 or 4) during the delivery of the baby;
- When the rupture could cause complications for the woman.
It is only possible to know if an episiotomy will be necessary during delivery!
The main controversy surrounding this procedure is the fact that many doctors perform it without the woman’s consent or simply to facilitate her labor.
However, despite this, it is a simple technique that does not need to be completely eliminated, as long as it is performed by a truly qualified professional. If the cut is made incorrectly, the woman may not be able to protect the anal sphincter (which is the main indication). Other consequences of episiotomy include pain, infection, bruising, and even rejection of the stitches.
Is it possible to avoid laceration?
The good news is that it is possible to reduce the chance of tearing and/or episiotomy. One alternative is to perform pelvic physical therapy throughout pregnancy.
Through exercise, the perineum, gluteal muscles, and hips are strengthened, giving women greater control over their genital region during childbirth.
These exercises can also use devices that stretch the vaginal canal and facilitate delivery.
A concept of childbirth that has been gaining a lot of attention is called humanized childbirth. The central idea is to let nature do its work at its own pace, that is, with minimal medical intervention.
Through this approach, women set their own pace and can choose to experience the moment in bed, in water, at home, or in the hospital.
Because there is no pressure, this type of childbirth demystifies the idea that it is a moment that requires some type of intervention, conveying the idea that it is a healthy and unique experience. In this type of childbirth, episiotomy is generally avoided as much as possible.
How to recover from a tear and/or episiotomy
If a tear is unavoidable, with or without an episiotomy, it is normal for some symptoms to arise, such as discomfort and pain when sitting. Ice packs are highly recommended to relieve the affected area. One tip is to wet the panty liner a little, leave it in the freezer, and then place it in your underwear for 15 minutes. This relieves pain, reduces swelling in the area, and facilitates healing.
Those who want to further activate recovery can take sitz baths with tea, such as:
- Stryphnodendron: Has antibacterial, analgesic, coagulant, anti-inflammatory, and astringent properties.
- Waybread: Its medicinal properties are healing, antiseptic, and anti-inflammatory;
- Marigold: Considered antibacterial, healing, sedative, and antiseptic.
If stitches are needed, your doctor may prescribe anti-inflammatory medication or analgesic sprays.
In addition, women are advised to take certain precautions, such as avoiding sexual intercourse for the first 40 days after delivery (the famous quarantine) and, if necessary, using pads, as in cases of hemorrhoids.
Now that you know what laceration and episiotomy are, it is up to you to seek alternatives to avoid overloading the perineum, strengthen the perineum during pregnancy, and discuss with your doctor all the possibilities for childbirth that apply to you.
The support of a doula and perinatal education are also extremely important in avoiding unnecessary episiotomies and other types of obstetric violence, as well as demystifying fears and empowering pregnant women in their choices. Information is essential for a birth in which the woman is the protagonist and can make conscious decisions.



0 Comments